






For decades, healthcare organizations have treated workforce readiness as a scheduled event. Annual competencies are completed. Documentation is filed. Leaders gain a sense of reassurance that teams are prepared for what lies ahead.
That model worked when care delivery was more predictable, roles were more static, and expectations changed slowly. But today’s environment no longer allows readiness to be something leaders check periodically and then set aside. In a system defined by staffing volatility, rising acuity, and constant change, readiness must hold under real conditions, not just at the moment it is assessed.
The challenge for nurse leaders is no longer proving that competency was validated. It is knowing, with confidence, that nurses can safely and effectively perform in the conditions they are facing right now.
Readiness Used to Be Predictable. Care No Longer Is.
The pace and complexity of healthcare delivery have shifted in ways that directly challenge traditional competency models. Staffing patterns change week to week. Nurses float more frequently across units. New technologies are introduced into daily practice. Patient populations are older and present with greater clinical complexity.
Yet competency validation has remained largely static, because it’s anchored to annual cycles and periodic checklists. The result is a growing mismatch between how care is delivered and how readiness is measured.
In a dynamic environment, skills can drift. Context changes. Confidence erodes quietly. And leaders are left relying on documentation that reflects a moment in time, rather than the reality of practice across shifts, units, and patient populations.
When the operating environment evolves faster than readiness models, assurance becomes an assumption.
Competency Is Not the Same as Confidence in Practice
Competency validation is necessary, but it is not sufficient.
Traditional competency processes often confirm exposure or completion: a module finished, a skill observed, a requirement met. Confidence in practice, however, reflects something different. It reflects whether skills are recent, reinforced, and applied in the right context.
From a leadership perspective, this distinction matters. Leaders are not asking whether a nurse has ever been validated. They are asking whether the team is prepared to perform safely today—on this unit, with this patient population, using this technology.
Without visibility between formal assessments, leaders have little insight into where confidence is strong and where it may be eroding. What fills that gap is assumption. And assumption is where both operational strain and risk quietly accumulate.
The Hidden Cost of Assumed Readiness
When readiness is measured infrequently, gaps do not disappear, they simply remain unseen.
Leaders may assume coverage is adequate, only to discover inconsistencies during a survey, an incident review, or a staffing transition. Teams may feel exposed rather than supported when expectations are unclear or unevenly validated. Educators and managers are left reacting instead of proactively addressing drift.
This is not a failure of intent. It is a visibility problem.
Assumed readiness concentrates risk in the moments leaders least expect such as during handoffs, high-acuity situations, onboarding surges, or cross-unit coverage. The organization may appear prepared on paper, while confidence in practice varies widely across the system.
How Leading Organizations Are Rethinking Readiness
More mature organizations are making a quiet but important shift: moving from episodic validation to continuous readiness management.
This does not mean more work or more assessments. It means better insight.
Organizations leading this shift share several operating practices:
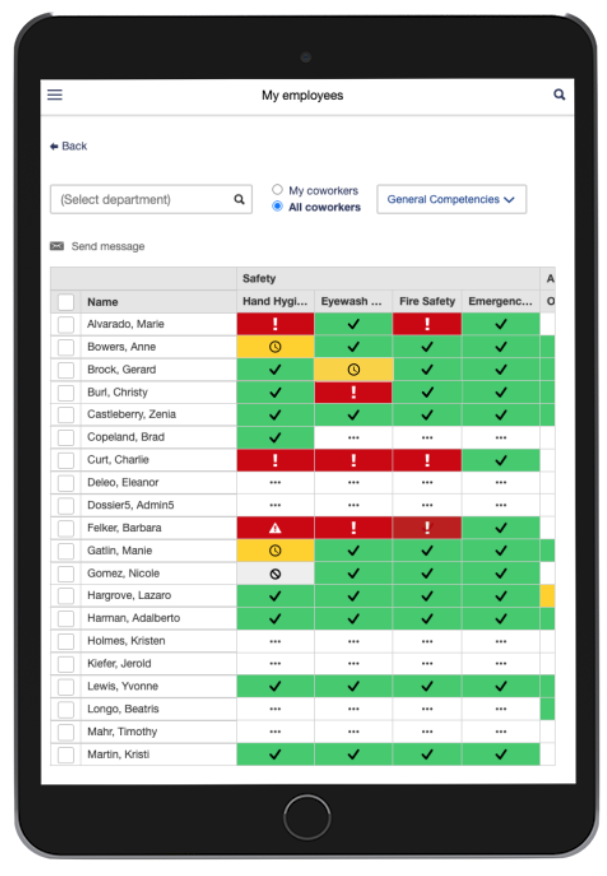
- Continuous visibility into competency status, rather than annual snapshots
- Standardized expectations across roles and units, reducing variability
- Early signal detection when skills drift or gaps emerge
- Actionable insight that supports leaders in real time, not just auditors
The goal is not to monitor more closely. The goal is to see sooner, respond earlier, and support teams before gaps become problems.
When readiness is embedded into operations, it becomes sustainable. When it is treated as an event, it becomes fragile.
What to Measure Instead of Completion
Completion alone tells leaders very little about readiness.
What builds confidence are leading indicators that reflect current conditions, such as:
- How recently high-risk skills were validated
- Where coverage gaps exist across units or roles
- How consistent expectations are across departments
- Which exceptions require leadership attention
These indicators allow leaders to answer readiness questions without scrambling and without relying on anecdote or assumption.
Confidence comes not from the volume of documentation, but from clarity.
Why This Matters Now
For nurse leaders, readiness underpins trust:
- Trust in staffing decisions.
- Trust in operational stability.
- Trust during regulatory review.
When leaders can see readiness clearly, they make decisions with greater confidence. Teams feel supported rather than scrutinized. Survey preparation becomes steadier and less reactive. Accountability is clearer, without becoming punitive.
Risk diminishes as confidence increases—not through tighter control, but through better visibility.
This shift also sets the foundation for future initiatives, including broader workforce analytics and nursing informatics efforts. Reliable readiness data is not just operationally useful; it becomes a strategic asset.
Platforms such as Dossier support this evolution by turning fragmented, manual competency records into structured, continuously updated data that leaders can trust—without adding unnecessary complexity.
Readiness Is an Operating Condition, Not an Event
Annual competency validation will always have a role in healthcare. But it can no longer carry the full weight of workforce readiness.
In modern care environments, readiness must be continuous, visible, and grounded in real practice, not just documented proof. Confidence in practice is what allows organizations to adapt, scale, and deliver safe care under pressure.
Workforce readiness isn’t something leaders confirm once a year.
It’s something they must be able to trust, every day.